On this page
What is rhinosinusitis?
Sinusitis is inflammation of the tissue that lines the sinuses.
Sinuses are hollow cavities found behind the nose, around the eyes and within the cheek bones.
Rhinitis is inflammation of the nasal airway.
The nose and sinus cavities are connected by narrow tubes, so inflammation can occur within both the sinuses and the nasal airway, known as rhinosinusitis.
Types of rhinosinusitis
What kind of rhinosinusitis you have depends on how long you have symptoms:

- Acute rhinosinusitis lasts up to 4 weeks.
- Subacute rhinosinusitis lasts between 4 and 12 weeks.
- Recurrent acute rhinosinusitis occurs 4 or more times a year, with each episode lasting at least 7 days.
- Chronic rhinosinusitis (CRS) lasts for 12 weeks or more.
Acute rhinosinusitis is common and occurs after a viral respiratory infection, such as the common cold.
CRS has a big effect on overall quality of life. CRS is an expensive disease for both the person who has it and the community. It leads to missed work and high total health care costs because it mostly affects people of working age.
CRS affects 5-10 percent of the population and is common in people who also have asthma or other allergic diseases.
Allergic rhinitis and chronic rhinosinusitis comparison
What are the differences between allergic rhinitis and chronic rhinosinusitis? Find out more.
Risk Factors for the Development of CRS
To keep your sinuses healthy, you need an immune system, a clearing system that works well, and open drainage pathways. Problems can be caused by many things, such as smoking, genetics, and severe acid reflux (when acid from your stomach goes up into your throat and sometimes your sinuses). The risk of CRS can also be changed by things in the environment that can affect the types of bacteria, viruses, and fungi that normally live in the nose and sinuses. It is very important that people who have both asthma and CRS take care of their asthma as well.
People more likely to get CRS are middle-aged and older adults, women, people who smoke (currently or in the past), people who are very overweight, or those who drink a lot of alcohol.
Symptoms of CRS
To be diagnosed with CRS, you must have at least two of the following symptoms for at least 12 weeks:
- blocked nose
- runny nose and post-nasal drip (where fluid drips from the sinuses and down the back of the nose into the throat causing people to clear their throat or cough)
- not being able to smell or only being able to smell very strong smells
- pressure and pain in the face
Symptoms can also be put into four groups depending on where they are located:
- Nose – problems include nasal blocking with discharge and a reduced sense of smell
- Face – such as pain, pressure, or a headache
- Oropharyngeal (mouth and throat) symptoms – such as ear pain, bad breath, post-nasal drip, a persistent cough, and toothaches
- Systemic (whole-body) signs – such as feeling sick and tired, because of the chronic inflammation process.
Blockage or obstruction of the nose is the most common symptom of CRS. Postnasal drip is the next most common.
Warning Signs or “Red Flags”
Symptoms and signs that suggest other conditions or complications that need urgent review:
- Facial pain or headaches without other signs of sinusitis
- High fever
- Nasal blockage or discharge on one side of nose only
- Symptoms that get worse, on one side
- Blood in nasal discharge
- Eye symptoms such as blurred or reduced vision
- Feeling numb or tingly in the face
- Facial swelling, causing the face to look uneven (facial asymmetry)
- Moderate to severe loss of sense of smell
Tests for diagnosis
Diagnosis of CRS is based on symptoms and test findings.
- Endoscopy (camera into the nose), may show abnormal tissue growths called nasal polyps, thick nasal discharge and swelling around sinus openings.
- CT scans may show swollen sinuses, mucous membranes, polyps, and blocked drainage of the sinuses.
Managing CRS
Medications, nasal irrigation (rinsing with a saltwater solution that can be bought at a pharmacy), and, in the worst cases, surgery, are all used to treat CRS. New biologic therapies, such as monoclonal antibody (disease-fighter) therapy, offer options for patients who have not responded to other treatments.
The following medicines may be tried by your doctor:

- Nasal rinses with a salt-water solution that reaches the sinuses.
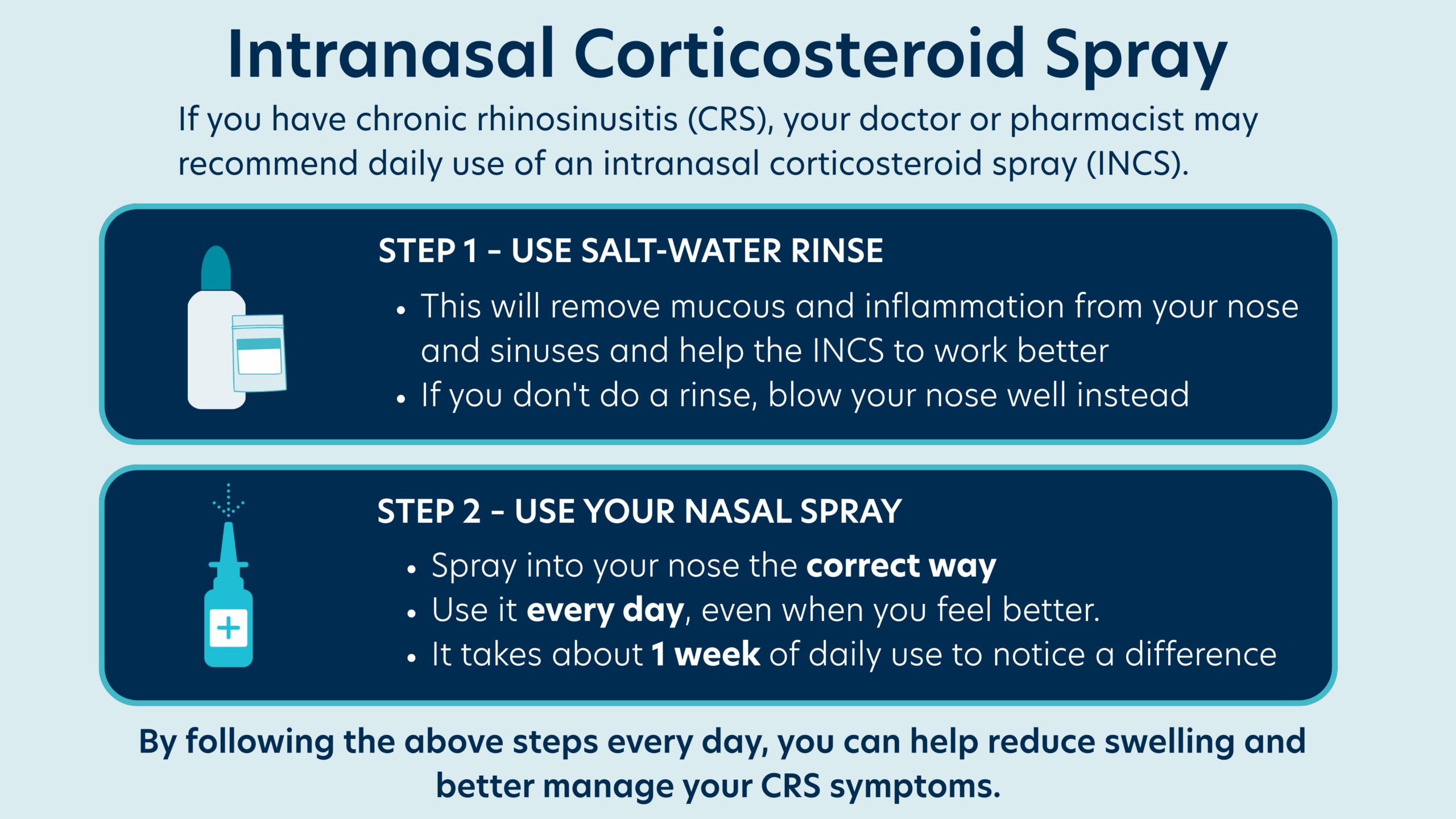
- Intranasal corticosteroid sprays (INCS), which are sprayed into the nose are used every day to help decrease swelling or inflammation. To work as they should they need to be sprayed into the nose in the right way. The INCS sprays only reach the nose and not the sinuses, unlike the nasal rinses.
- Oral corticosteroid drugs may help for a short time, but they can be problematic if used often and/or for a long time.
- Antibiotics to treat infection.
- Leukotriene antagonists can stop some of the proteins that cause inflammation.
- Aspirin desensitisation therapy can be an option for people who are allergic to anti-inflammatory drugs such as Nurofen, Brufen, Indocid and aspirin.
Surgery:
If a person has tried the medicines their doctor has prescribed and they haven’t helped, they may be referred to an ENT (Ear, Nose and Throat) surgeon for possible nose and sinus surgery. Nasal polyps can block the nose and sinuses and are often removed to improve nose and sinus drainage.
Goals of surgery:

- Improving breathing through the nose and drainage of the nose and sinuses so that medications and nasal rinses can work better.
- Removing polyps (abnormal growths), fungal or mucus build-up
- Keeping the lining of the nose and sinuses in a good condition
Nasal rinses are a permanent treatment for people who have sinus surgery.
Treatment with monoclonal antibodies
Some people who have ongoing symptoms even though they follow specialist advice and have had surgery for nasal polyps can be reviewed by their specialist for possible treatment with monoclonal antibodies. Monoclonal antibodies are immune proteins that are made in a laboratory and are targeted to block the inflammatory molecules causing CRS.
There are strict guidelines that must be followed for prescribing monoclonal antibody treatment. It is a high-cost treatment and can only be used in those who fulfil certain criteria.
Summary

- CRS is a medical condition that needs to be treated by a doctor.
- For people with CRS, management may include trying different medicines, treatments and/or surgery.
- There is no cure for CRS yet, but the treatments available can make life a lot better.
- If CRS is still not well managed after medical and surgical treatment, and is affecting your family, work and social life, monoclonal antibody treatment may be an option.
- When trying to manage CRS, it’s important to follow your doctor’s instructions.
Webinars
Related information
FAQs
-
The type of rhinosinusitis you have depends on how long your symptoms last:
- Acute rhinosinusitis lasts up to 4 weeks and often happens after a cold or other viral infection.
- Chronic rhinosinusitis (CRS) lasts for 12 weeks or more. It is a long-term condition that affects about 5-10 percent of people and is common in people with asthma and allergies.
-
- Problems with the structure of the cartilage tissue in the nose (such as a deviated septum)
- Smoking
- Nasal polyps
- Overuse of decongestant nasal sprays
- Allergies such as allergic rhinitis, especially if untreated or poorly controlled
- Being overweight
- Drinking a lot of alcohol
- Being middle aged
- Being female
-
Chronic rhinosinusitis (CRS) can have a big impact on a person’s quality of life and mental health and can lead to decreased physical and social activity. It also impacts the wider community by increasing healthcare costs for things like doctor visits, medicine, and surgery. As it mostly affects people of working age, it can lead to missed work and lower productivity.
CRS is less common in children, but it can affect their concentration and academic performance.
-
Chronic rhinosinusitis (CRS) is more common in adults and becomes more likely to develop as people get older. It affects 5- 10 percent of people.
-
The most common symptoms of chronic rhinosinusitis (CRS) are blocked nose and post-nasal drip (mucus dripping down the back of the throat).
You may have CRS if you’ve had two or more of these symptoms for at least 12 weeks:
- blocked nose on both sides
- runny nose from both nostrils and post-nasal drip
- not being able to smell or only being able to smell strong smells
- pressure and pain in the face
See a doctor urgently if you have any of these symptoms, as they may be caused by something more serious:
- Facial pain or headaches without other signs of sinusitis
- High fever
- Blocked nose or discharge on one side of nose only
- Symptoms that are worse on one side
- Blood in nasal mucus
- Eye symptoms such as blurred or reduced vision
- Numbness or tingling in the face
- Facial swelling, causing the face to look uneven (facial asymmetry)
- Moderate to severe loss of sense of smell
-
Diagnosis of chronic rhinosinusitis (CRS) is based on symptoms and test findings.
- Endoscopy (camera into the nose) may show abnormal tissue growths called nasal polyps, thick nasal discharge and swelling around sinus openings.
- CT scans may show swollen sinuses, mucous membranes, polyps, and blocked drainage of the sinuses.
-
Skin prick tests are not used to diagnose chronic rhinosinusitis (CRS). Skin prick tests can be used to help diagnose allergic rhinitis. They can show if you’re sensitised to things like dust mites and pollen which can cause allergic rhinitis, but this isn’t the cause of CRS.
-
People with chronic rhinosinusitis (CRS) can manage it in a few different ways:
- Medical treatment – This usually includes nasal rinses (salt-water solutions) and daily intranasal corticosteroid sprays to reduce swelling. Antibiotics may be prescribed if there’s an infection, and sometimes a short course of oral steroids is given.
- Surgery – If medications don’t help, surgery might be needed to clear blockages and fungal buildup, remove polyps, and improve sinus drainage and breathing.
- Monoclonal antibody therapy – For people with ongoing symptoms, even after medicine and surgery, a specialist may consider this advanced treatment. It’s only available to those who meet set requirements.
-
If a person has symptoms of chronic rhinosinusitis (CRS), they should see their GP. The GP will decide, based on the history and signs and symptoms, whether they can manage the patient themselves or whether the patient needs a referral to an allergist or an ear, nose and throat (ENT) surgeon.
-
There’s no cure for chronic rhinosinusitis (CRS), but treatments can help manage the symptoms and improve your quality of life.
-
Nasal polyps are soft, painless, non-cancerous growths in the nose or sinuses, usually shaped like teardrops. They often form where the upper sinuses drain into the nose.
People with long-term sinus inflammation may develop them. About 20–30 percent of people with chronic rhinosinusitis (CRS) get nasal polyps, which can impact quality of life and mental health.
They can be diagnosed with a nose camera (endoscopy) or a CT scan.
-
People with nasal polyps can see an ENT surgeon for surgery to remove the polyps. This helps improve sinus drainage, so medicines and nasal rinses work better.
After surgery, it’s important to keep using nasal rinses to keep the sinuses clear.
Surgery removes nasal polyps, but they may grow back because surgery doesn’t treat the underlying cause of chronic rhinosinusitis (CRS). If the polyps return, you can talk to your specialist about other treatment options, such as monoclonal antibody therapy. This is an expensive treatment that is only prescribed by allergy specialists to patients who meet set requirements.
-
No. Some people only have allergic rhinitis, and some people only have chronic rhinosinusitis (CRS). Some people have both. Untreated or poorly controlled allergic rhinitis can increase the risk of developing CRS.
-
Properly managing allergic rhinitis can help lower the risk of developing chronic rhinosinusitis (CRS). If allergic rhinitis is left untreated, this can increase the risk of CRS due to chronic inflammation of the nasal airway which reduces the normal mucus drainage from the sinuses, leading to a risk of bacterial overgrowth and infection.