
Rhinitis
Rhinitis is inflammation of the nasal airway.
- Allergic rhinitis (AR), commonly known as hay fever, is triggered by exposure to allergens, such as grass pollens, dust mite or animal dander.
- Allergic rhinoconjunctivitis is the name given if the patient has symptoms affecting the eyes as well as the nose. This occurs in 70% of patients with allergic rhinitis.
- Non-allergic rhinitis is rhinitis that is not triggered by allergen exposure but is due to other causes such as smoke or changes in temperature.
Sinusitis
Sinusitis is inflammation of the tissue that lines the sinuses.
Sinuses are hollow cavities found behind the nose, around the eyes and within the cheek bones. The nose and sinus cavities are connected by narrow tubes, so inflammation can occur within both the sinuses and the nasal airway, known as rhinosinusitis.
There are different types of sinusitis, depending on how long the symptoms last.
- Acute rhinosinusitis lasts up to 4 weeks
- Subacute rhinosinusitis lasts between 4 and 12 weeks
- Chronic rhinosinusitis (CRS) lasts for 12 weeks or more.
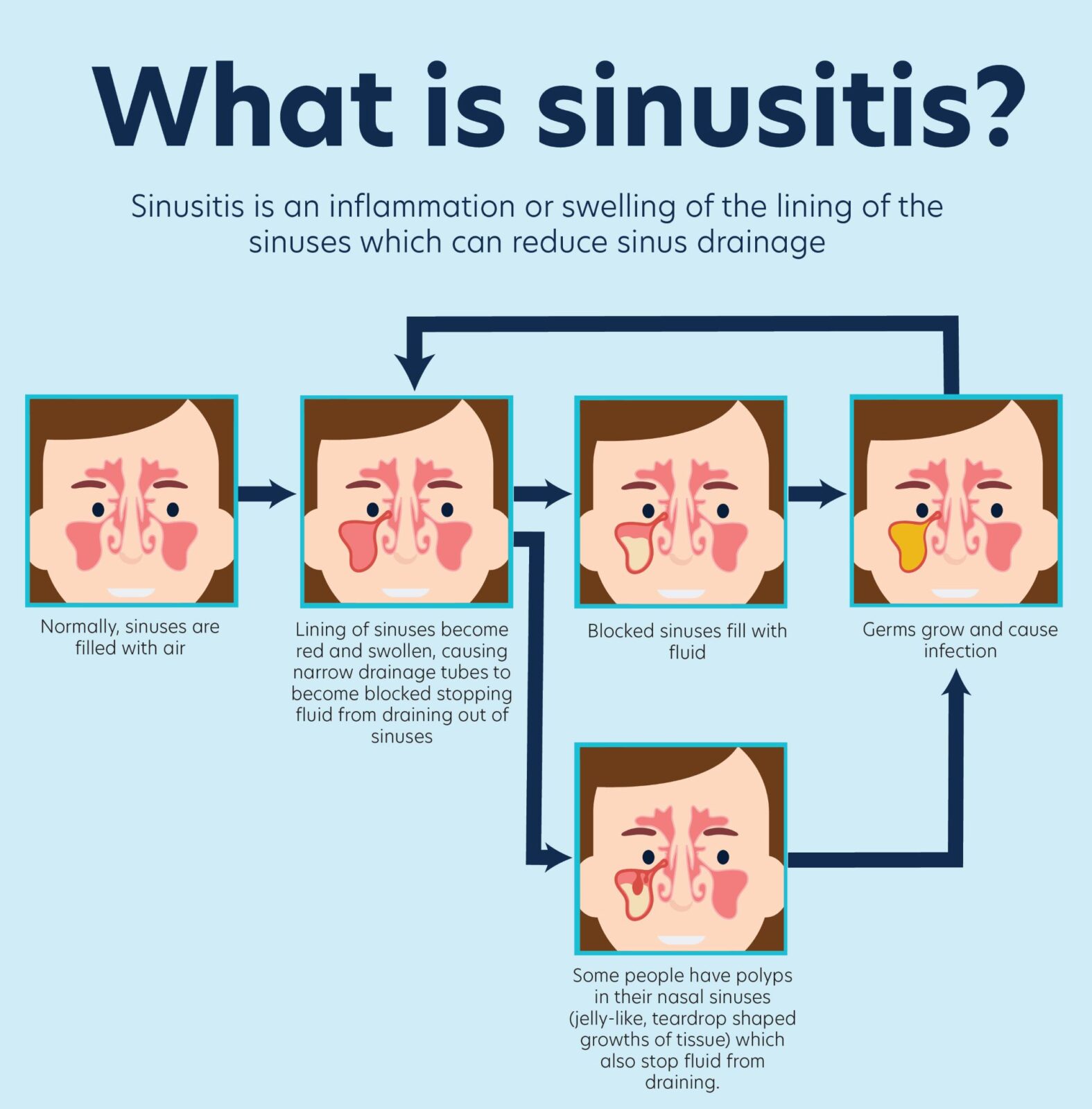
The sinuses produce fluid (mucus) which drains out of the narrow passages into the nose. When there is inflammation of the nasal or sinus tissue, the narrow tubes become blocked. This stops mucus draining out of the nose causing pain and discomfort in the face as the pressure inside the sinuses increases. When the tubes become blocked and mucus cannot drain from the sinuses, bacteria can become trapped in the sinus cavities causing what is known as a secondary bacterial infection.
Some patients with CRS also have nasal polyps which are soft, non-cancerous growths that develop on the lining of the sinuses or nose. Large nasal polyps can also contribute to an increased fluid in the sinuses.
Patients with CRS can also have allergic rhinitis, but many people with CRS do not have allergy as the main cause of their symptoms. Chronic sinusitis more commonly affects adults rather than children. Untreated allergic rhinitis can increase the risk of CRS due to chronic inflammation of the nasal airway which reduces the normal mucus drainage from the sinuses, leading to a risk of bacterial overgrowth and infection.
Allergic rhinitis and chronic rhinosinusitis: table comparison
Clinical features:
| CLINICAL FEATURES | Allergic rhinitis (hay fever) | Chronic rhinosinusitis (CRS) |
|---|---|---|
| Nose affected | Yes | Yes |
| Sinuses affected | No | Yes |
| Runny nose vs nasal blockage | Both | Nose more blocked than runny |
| Sneezing, Nasal itch | Yes | Uncommon |
| Nasal discharge | Often clear | Often thick, yellow (purulent) |
| Throat clearing, coughing, postnasal drip (mucus dripping down back of throat) | Yes (throat itch) | Yes |
| Sense of smell | Can be reduced but often OK | Reduced or absent |
| Growths in the nose (nasal polyps) | No | May be present |
| Headache, head pressure | Uncommon (may complain of brain fog) | Yes |
| Face pain | No | Yes |
| Infection/need for antibiotics possible | No | Yes |
| Disturbed sleep | Yes | Yes |
| Watery, itchy eyes | Yes (if associated allergic conjunctivitis) | No |
| Timing of symptoms through the year | Can be seasonal (e.g. grass pollen allergy occurs mainly in spring and summer) or all year round (e.g. dust mite allergy) | Not usually seasonal, but more frequent infections are possible in winter. If also have allergic rhinitis, can have symptoms at other times. |
| Associated with asthma | Yes, usually asthma that starts in childhood | Yes, usually asthma that starts in adulthood or ‘eosinophilic’ asthma |
| Intolerance of aspirin, anti-inflammatory medications (NSAIDs) | No | Can be present |
Tests:
| TESTS | Allergic rhinitis (hay fever) | Chronic rhinosinusitis (CRS) |
|---|---|---|
| Skin Prick Test or Blood Test for environmental allergens such as dust mite or grass | Usually positive | May be positive to allergens but allergens do not cause the condition |
| CT Scan | Not needed | May be needed |
| Nasoendoscopy (camera into the nose) | Not needed | May be needed |
Treatment:
| TREATMENT | Allergic rhinitis (hay fever) | Chronic rhinosinusitis (CRS) |
|---|---|---|
| Reduce exposure to triggers, such as grass or dust | Yes | Yes |
| Steroid nasal spray | Yes | Yes |
| Saline (salt) nasal sprays or rinses | Yes | Yes |
| Antihistamines | Yes Nasal sprays work better than tablets | May not work |
| Combined steroid and antihistamine nasal sprays | Yes | Yes |
| Oral steroids | No | Sometimes (short course only) |
| Allergen immunotherapy (Desensitisation) | Often works | May not work |
| Monoclonal Antibodies | No | May work if there are nasal polyps |
| Antibiotics | No | Sometimes |
| Surgery | No | May be needed |
Referral to:
| REFERRAL TO | Allergic rhinitis (hay fever) | Chronic rhinosinusitis (CRS) |
|---|---|---|
| Allergy specialist | Yes If severe and to consider allergen immunotherapy | Yes to check for allergens and consider medications |
| Ear Nose Throat Surgeon | No | Yes to consider nasoendoscopy and surgery |
The chronic rhinosinusitis and allergic rhinitis comparison has been created by Allergy & Anaphylaxis Australia thanks to an unrestricted educational grant from GSK.