Updated September 2024
On this page
If you or the person you are with are showing any signs of a severe allergic reaction
Knowing what to do in an emergency is an important part of allergy care.
Being prepared can help you feel more in control and confident in managing anaphylaxis. Allergy & Anaphylaxis Australia has a lot of helpful information and resources to help you do this.
Signs and symptoms of anaphylaxis
Most allergic reactions are mild or moderate, but some mild to moderate allergic reactions can quickly worsen to anaphylaxis.
BUT remember – mild or moderate allergic symptoms may not always occur before symptoms of anaphylaxis.
Learn about signs and symptoms of an allergic reaction (including anaphylaxis)
Signs and symptoms video
ASCIA Action Plans
Learn about the different types of ASCIA Action Plans and how to follow them during an allergic reaction.
Positioning
Positioning (whether a person is lying, sitting or standing) is a very important part of managing anaphylaxis.
The person must lay flat (or, if breathing is difficult, they can sit with legs outstretched).
Correct positioning is the first action (instruction) on the ASCIA Action Plan yet many people don’t think of it as part of managing anaphylaxis which is a medical emergency.
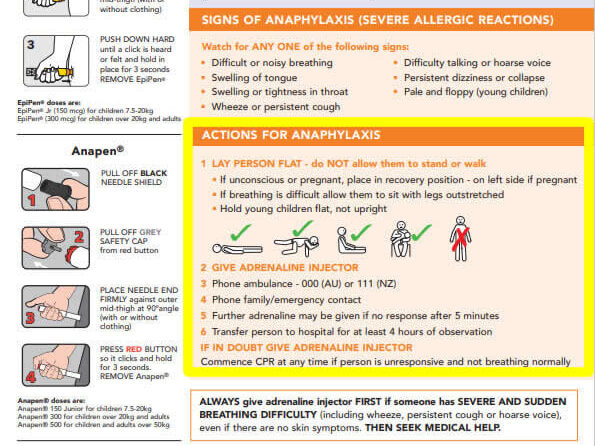
If someone is having anaphylaxis:
LAY PERSON FLAT – do NOT allow them to stand or walk
Lay person flat

Do not allow them to stand or walk

If breathing is difficult allow them to sit with legs outstretched

Hold babies and young children flat, not upright

If unconscious or pregnant, place in recovery position – on left side if pregnant
How to position a child or adult having anaphylaxis
This animation was developed by the National Allergy Council.
Importance of laying down during anaphylaxis
Dr Paxton Loke – Paediatric Allergist and Immunologist from the Murdoch Children’s Research Institute and Melbourne Allergy Centre and Children’s Specialists Medical Group.
Adrenaline (epinephrine) devices
ADRENALINE IS LIFE SAVING medication for someone having a severe allergic reaction known as anaphylaxis.
An adrenaline device contains one dose of adrenaline and is designed to be used by people who are not medically trained.
There are two different brands available in Australia – Anapen® and EpiPen®.
People prescribed an adrenaline device should have one available to them at all times. They should keep a copy of their ASCIA Action Plan for Anaphylaxis with their adrenaline device.
Instructions on how to give the adrenaline device are on each device and on the ASCIA Action Plan for Anaphylaxis and the ASCIA First Aid Plan for Anaphylaxis. A&AA has videos on how to give adrenaline devices below.
How to give an Anapen®
Remember: White end on leg, press thumb on red
How to give an EpiPen®
Remember: Blue to the sky, orange to the thigh
How adrenaline works during anaphylaxis
Dr Paxton Loke – Paediatric Allergist and Immunologist from the Murdoch Children’s Research Institute (MCRI) and Melbourne Allergy Centre and Children’s Specialists Medical Group

Is it asthma or anaphylaxis?
ALWAYS give adrenaline device FIRST, and then asthma reliever puffer if someone with known asthma and allergy to food, insects or medication (who may have been exposed to the allergen) has SUDDEN BREATHING DIFFICULTY (including wheeze, persistent cough or hoarse voice) even if there are no skin symptoms.
If it turns out that you were having asthma and not anaphylaxis, giving an adrenaline device is not dangerous for people having asthma and can help as it opens airways making breathing easier.
Hear what Dr Preeti Joshi has to say about asthma and anaphlaxis.
If in doubt, give the adrenaline device.
Other important things to remember:

DO NOT SHOWER when you have anaphylaxis.
Showering during anaphylaxis can make a person more unwell. People sometimes get in the shower to help relieve skin symptoms which feel itchy or hot. Standing up and showering during anaphylaxis can cause or worsen a drop in blood pressure and lead to collapse. Follow instructions on the ASCIA Action Plan. If the skin feels itchy or burning, use a cold wet cloth to help cool the skin while you wait for an ambulance.

Antihistamines DO NOT stop anaphylaxis.
Antihistamines only help with mild/moderate symptoms like itching or swelling of the face, lips and eyes.
Anaphylaxis training
Be aware that not all first aid courses cover the management of anaphylaxis well. The Australasian Society of Clinical Immunology & Allergy (ASCIA) has free online training courses on anaphylaxis for the community, schools and childcare, and health professionals. Even if you are required to do a first aid course through a registered first aid training provider for your workplace or community organisation, A&AA recommend also doing the ASCIA anaphylaxis e-training as this training often contains more information on avoiding allergens and emergency treatment of anaphylaxis.

Mobile phone coverage
In Australia, mobile phone coverage varies between providers. When choosing a mobile phone provider, consider whether they have coverage in areas you travel to so you will be able to call for help easily in an emergency.